Tipranavir
- CAS NO.:174484-41-4
- Empirical Formula: C31H33F3N2O5S
- Molecular Weight: 602.66
- SAFETY DATA SHEET (SDS)
- Update Date: 2024-11-17 16:00:36
What is Tipranavir?
Absorption
Absorption is limited, although no absolute quantification of absorption is available.
Toxicity
Oral LD50 in rat is over 5,000 mg/kg. Side effects include thirst and hunger, unexplained weight loss, increased urination, fatigue, and dry, itchy skin.
Description
Tipranavir, an oral non-peptidic HIV protease inhibitor, was granted accelerated approval for use in combination with ritanovir and was subsequently launched the same month in 2005. The targeted patient population includes HIV-1 infected adults with evidence of viral replication and demonstrated resistance to multiple protease inhibitors. As with other protease inhibitors, binding at the HIV-1 protease’s active site inhibits the virus-specific processing of the Gag and Gag-Pol polyproteins in HIV-1-infected cells resulting in the production of non-infectious virions. An effective regimen to reduce viral load and to preserve immune function typically consists of a cocktail of a protease inhibitor and at least one nucleoside reverse transcriptase inhibitor. It is believed that tipranavir has been effective where other protease inhibitors have encountered resistance because, as a non-peptidic inhibitor, it was designed by structure-based analysis to have increased flexibility making it acquiescent to conformational alterations at the binding site. Boosting with ritonavir (200 mg) increased tipranavir Cmin 4-fold and Cmax 20-fold. The primary route of excretion is through the feces (83%) with an effective mean elimination half-life of 4.8 h in healthy volunteers and 6.0 h in HIV-infected adults. The efficacy of tipranavir/ritonavir combination therapy has been evaluated in multiple clinical trials. In general, the adverse events included nausea, vomiting, and diarrhea. While tipranavir is a CYP3A4 inducer and substrate, as previously stated, its co-administration with the CYP3A4 inhibitor ritonavir results in net inhibition; therefore, patients should avoid the concomitant use of drugs highly dependent on CYP3A4 for clearance. The complete list of contraindicated drugs can be found in the package insert, but the general classes include antiarrhythmics, antihistamines, antimycobacterials, neuroleptics, sedatives, ergot derivatives, GI motility agents, and the herbal supplement St. John’s wort. Finally, as the elevated liver enzyme levels suggest, tipranavir should not be taken by patients with severe liver disease. Patients with clinical symptoms of hepatitis should immediately discontinue use of tipranavir. It is highly recommended that liver function tests be performed prior to treatment and throughout the course of therapy.
Chemical properties
White Solid
Originator
Pharmacia &Upjohn (US)
The Uses of Tipranavir
Nonpeptidic HIV protease inhibitor (NPPI). Antiviral
The Uses of Tipranavir
Nonpeptidic HIV protease inhibitor (NPPI). Antiviral.
What are the applications of Application
Tipranavir is a nonpeptidic protease inhibitor and antiviral agent
Background
Tipranavir is a sulfonamide-containing dyhydropyrone and a nonpeptidic protease inhibitor that targets the HIV protease. Tipranavir and ritonavir are coadministered to treat HIV.
Indications
For combination antiretroviral treatment of HIV-1 infected adult patients with evidence of viral replication, who are highly treatment-experienced or have HIV-1 strains resistant to multiple protease inhibitors.
Definition
ChEBI: A pyridine-2-sulfonamide substituted at C-5 by a trifluoromethyl group and at the sulfonamide nitrogen by a dihydropyrone-containing m-tolyl substituent. It is an HIV-1 protease inhibitor.
brand name
Aptivus
Acquired resistance
In a study of 105 viruses resistant to other protease inhibitors, 90% exhibited a more than four-fold decrease in susceptibility and 2% high-level resistance (>10-fold decrease). The predominant emerging mutations in use with ritonavir are L33F/I/V, V82T/L and I84V. Combination of all three of these mutations is usually required for reduced susceptibility. Mutations at positions 47, 58 and 74 are also associated with resistance.
General Description
Tipranavir is unique among the PIs because it is not a peptidomimeticcompound. It does appear to bind to the activesite of HIV-1 protease the same as the peptidomimetics do.The benefit of this agent is that, because it is a differentchemical structure, cross-resistance does not develop tothe same extent as seen with the peptidomimetics. Thedrug is administered with a booster dose of ritonavir. Thisprotocol inhibits CYP3A4, causing the levels of tipranavirto increase.
Pharmaceutical Applications
A non-peptidic protease inhibitor formulated as capsules or solution for oral use.
Mechanism of action
Tipranavir appears to be bound to the same active site of HIV-1 protease as the peptidomimetics are, but because of its different chemical structure, cross-resistance is significantly less than that seen between the peptidomimetics. The drug suppresses viral replication in various strains of HIV-1 in vitro, and when combined with azothymidine or delaviridine, synergistic activity is noted in vitro. Tipranavir has an advantage over the other PIs in that it is not as strongly bound to plasma protein as the earlier PIs are, a property that reduces the 90% inhibition concentration.
Pharmacokinetics
Tipranavir is a non-peptidic protease inhibitor (PI) of HIV. Protease inhibitors block the part of HIV called protease. HIV-1 protease is an enzyme required for the proteolytic cleavage of the viral polyprotein precursors into the individual functional proteins found in infectious HIV-1. Nelfinavir binds to the protease active site and inhibits the activity of the enzyme. This inhibition prevents cleavage of the viral polyproteins resulting in the formation of immature non-infectious viral particles. Protease inhibitors are almost always used in combination with at least two other anti-HIV drugs.
Pharmacokinetics
Oral absorption: Not known/available
Cmax 500 mg + 200 mg ritonavir twice: c. 57.2 mg/L (female);
daily: 46.8 mg/L (male)
Cmin 500 mg + 200 mg ritonavir twice: c. 25.1 mg/L (female);
daily: 21.5 mg/L (male)
Plasma half-life: c. 5.5 h (female); 6 h (male)
Volume of distribution: Not known/available
Plasma protein binding: >99.9%
Absorption and distribution
The combination with ritonavir may be taken with or without food. No studies have been conducted to determine the distribution into human CSF, semen or breast milk.
Metabolism and excretion
Metabolism in the presence of 200 mg ritonavir is minimal. Around 82% is excreted in the feces and 4% in the urine. In mild hepatic impairment it should be used with caution; it should not be used in moderate or severe hepatic impairment.
Clinical Use
Treatment (in combination with other antiretroviral drugs) of HIV-1 infection in patients unresponsive to more than one other protease inhibitor
Side Effects
Adverse effects include nausea, vomiting, diarrhea, fatigue and headache. In studies of ritonavir-boosted regimens higher rates of hepatotoxicity have been observed with tipranavir than with other protease inhibitors. In addition, 14 reports of intracranial bleeding (eight fatal cases) associated with tipranavir have been reported. It has been associated with dyslipidemia to a greater extent than other protease inhibitors.
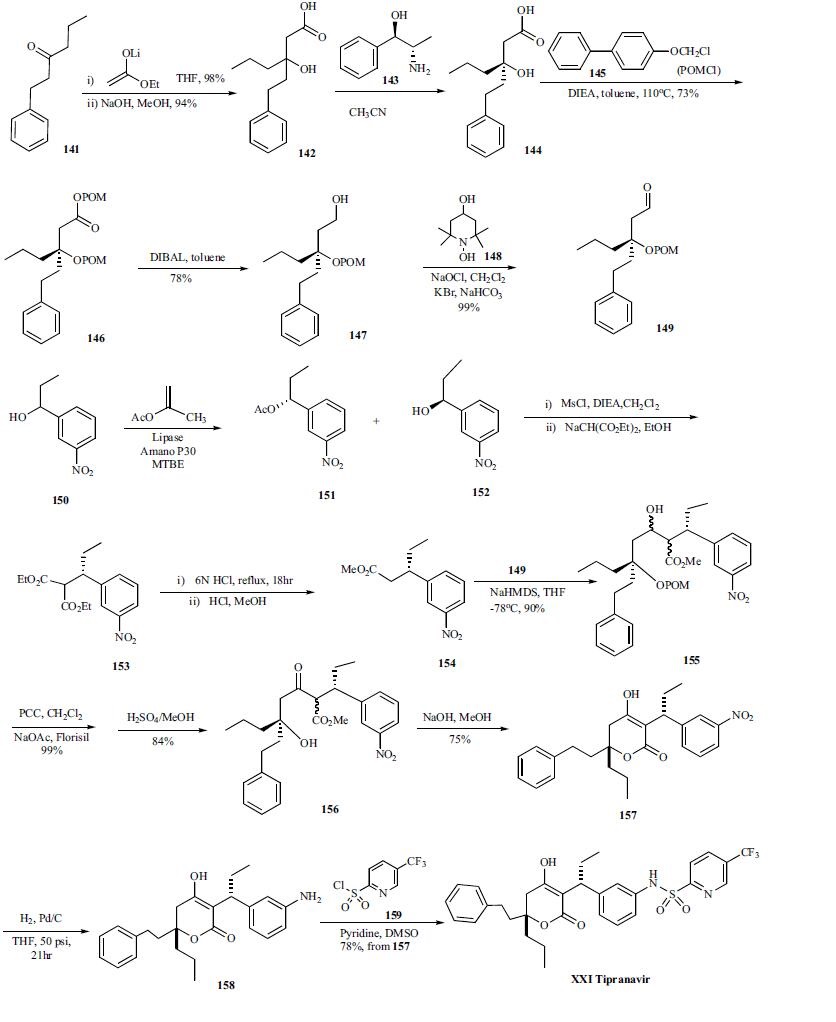
Synthesis
Synthesis of tipranavir was assembled by an aldol condensation between two chiral key intermediates, 149 and 154. Condensation of 1-phenylhexan-3-one (141) with ethyl acetate in the presence of butyllithium and diisopropylamine in THF gave racemic 3-hydroxy-3-(2-phenylethyl)hexanoic acid ethyl ester, which was directly hydrolyzed with NaOH in methanol to corresponding free acid 142 in 94% yield. The racemic 142 was subjected to optical resolution with (1R, 2S)-(-)-norephedrine to yield chiral compound 144 which was alkylated with 4-biphenylyloxymethyl chloride (POMCl) and diisopropylethylamine in toluene to give POM protected ester 146 in 73% yield . The choice of POM protection group is for the purification since the POM protected intermediates were highly crystalline compounds. The ester group of 146 was reduced with diisobutylaluminum hydride in toluene to give corresponding alcohol 147 in 78% yield, which was oxidized with 4-hydroxy-2,2,6,6-tetramethylpiperidinyloxy radical (TEMPO)/bleach (NaOCl) to yield corresponding aldehyde 149 in 99% yield. The other chiral intermediate 154 was synthesized as described below. Racemic compound 150 was subjected to kinetic enzymatic resolution with a lipase and isopropenyl acetate in dichloromethane to give chiral alcohol 152 which was converted to its mesylate and reacted with sodium diethyl malonate to give diester 153. The diester 153 was decarboxylated under an acid condition and re-esterified to give optical pure intermediate 154. Aldol condensation of 149 and 154 with sodium hexamethyldisilazide in THF at low temperature gave hydroxyester 155 in 90% yield as a mixture of four diastereomers. This mixture was oxidized with pyridinium chlorochromate (PCC) in dichloromethane to afford corresponding ketoester which was subsequently treated with sulfuric acid in methanol to remove the POM protecting group to yield hydroxy ketoester 156 in 84% yield. Compound 156 was cyclized with NaOH in methanol/water to afford dihydropyranone 157 in 75% yield. The nitro group of 157 was reduced with hydrogen over Pd/C in THF to give corresponding aniline 158, which was finally amidated with 5-(trifluoromethyl)pyridine-2- sulfonyl chloride 159 and pyridine in DMSO to give tipranavir (XXI) in 78% yield from compound 149.
Drug interactions
Potentially hazardous interactions with other drugs
Antacids: avoid giving for 2 hours after tipranavir
administration.
Antibacterials: plasma concentration of clarithromycin
and other macrolides increased - reduce dose of
clarithromycin in renal impairment; concentration
increased by clarithromycin; rifabutin concentration
increased (risk of uveitis) - reduce dose; concentration
possibly reduced by rifampicin - avoid; avoid with
telithromycin in severe renal and hepatic failure.
Anticoagulants: avoid with apixaban and rivaroxaban.
Antidepressants: concentration possibly reduced by
St John’s wort - avoid.
Antimalarials: use artemether/lumefantrine with
caution; concentration of quinine increased.
Antipsychotics: possibly increases aripiprazole
concentration - reduce aripiprazole dose; possibly
increases quetiapine concentration - avoid.
Antivirals: reduces concentration of abacavir,
dolutegravir, didanosine, fosamprenavir, lopinavir,
saquinavir and zidovudine; concentration increased
by atazanavir, also concentration of atazanavir
reduced; concentration reduced by etravirine, also
concentration of tipranavir increased - avoid.
Beta-blockers: avoid with metoprolol for heart failure.
Ciclosporin: levels possibly altered by tipranavir.
Cobicistat: concentration of both drugs reduced -
avoid.
Lipid-lowering drugs: increased risk of myopathy
with atorvastatin, max dose 10 mg; avoid with
lomitapide; concentration of rosuvastatin increased
- reduce rosuvastatin dose; concentration of
simvastatin increased - avoid.1
Orlistat: absorption possibly reduced by orlistat.
Ranolazine: possibly increases ranolazine
concentration - avoid.
Sirolimus: levels possibly altered by tipranavir.
Tacrolimus: levels possibly altered by tipranavir.
Ulcer-healing drugs: concentration of esomeprazole
and omeprazole reduced.
Metabolism
Hepatic. In vitro metabolism studies with human liver microsomes indicated that CYP 3A4 is the predominant CYP enzyme involved in tipranavir metabolism.
Metabolism
Tipranavir is metabolised by the cytochrome P450 system (mainly the isoenzyme CYP3A4), although when given with ritonavir metabolism is minimal with the majority of tipranavir being excreted unchanged in the faeces.
Properties of Tipranavir
| Melting point: | 86-890C |
| alpha | D +20° (ethanol) |
| Boiling point: | 712.3±70.0 °C(Predicted) |
| Density | 1.313±0.06 g/cm3(Predicted) |
| storage temp. | -20°C Freezer |
| solubility | Methanol (Slightly) |
| form | Solid |
| pka | 4.50±1.00(Predicted) |
| color | White to Pale Yellow |
Safety information for Tipranavir
Computed Descriptors for Tipranavir
New Products
Tert-butyl bis(2-chloroethyl)carbamate (S)-3-Aminobutanenitrile hydrochloride N-Boc-D-alaninol N-BOC-D/L-ALANINOL 3-(2,4-Dimethoxybenzyl)dihydropyrimidine-2,4(1H,3H)-dione 7-Bromo-1H-indazole N-octanoyl benzotriazole 3,4-Dibenzyloxybenzaldehyde 4-Hydrazinobenzoic acid Electrolytic Iron Powder Fmoc-Val-Cit-PAB 1,1’-CARBONYLDIIMIDAZOLE R-2-BENZYLOXY PROPIONIC ACID 4-HYDROXY BENZYL ALCOHOL 1,1’-CARBONYLDI (1,2-4 TRIAZOLE) S-2-CHLORO PROPIONIC ACID (2-Hydroxyphenyl)acetonitrile 4-Bromopyrazole 5-BROMO-2CYANO PYRIDINE 5,6-Dimethoxyindanone 5-broMo-2-chloro-N-cyclopentylpyriMidin-4-aMine 1-(4-Methylphenylsulfonyl)-1H-1,2,3-benzotriazole 1-(2-Chlorobenzyl)-4-nitro-1H-pyrazole 1-(2-Nitrophenyl)-4-phenylpiperazineRelated products of tetrahydrofuran
![[13C6]-Tipranavir](https://img.chemicalbook.in/)
You may like
-
 Tipranavir CAS 174484-41-4View Details
Tipranavir CAS 174484-41-4View Details
174484-41-4 -
55441-95-7 2 2-BIS(2-HYDROXYETHOXY)-1 1-BINAPHTHYL 99%View Details
55441-95-7 -
Ste-Glu-AEEA-AEEA-OSUView Details
1169630-40-3 -
1446013-08-6 Fmoc-His-Aib-OH TFA 98%View Details
1446013-08-6 -
127464-43-1 99%View Details
127464-43-1 -
Chloro Uracil 99%View Details
1820-81-1 -
2-ETHYLPYRIDINE 100-71-0 99%View Details
100-71-0 -
13162-05-5 99%View Details
13162-05-5